| |
When was the last time you stopped to smell the roses? Its a common expression, but we mean this literally.
Our sense of smell is such an important part of daily life that we often fail to appreciate it. While you may not have actually smelled any roses lately, you would certainly know if you were unable to do so.
Indeed, for about 21 million people in the United States who experience some type of abnormal smell function, a sense of smell is nothing to take for granted. While the loss of smell may not seem as disabling as loss of vision or hearing, smell loss can significantly interfere with quality of life in our enjoyment of food and social situations. Moreover, as Dr. Robert Henkin has shown in his long scientific career, our understanding of the processes leading to abnormal smell function and its treatment has important implications for a variety of other conditions, including chronic stress and neurological and inflammatory diseases.
Our understanding of the processes leading to abnormal smell function and its treatment has important implications for a variety of other conditions, including chronic stress and neurological and inflammatory diseases.
Since 1969, Dr. Henkin has led the Taste and Smell Clinic in Washington, DC. It is devoted to helping patients with taste and smell loss. In the Clinics beginning years, Dr. Henkin and his colleagues developed a specific methodology for testing a patients level of smell and taste perception.
There are many known classes of smell, including pungent, putrid, sweet, minty, flowery, fruity, and ether-like. For each class, the patient was given a compound to smell and the scientists recorded the concentration at which the patient noticed the scent. Based on this concentration, the researchers were able to classify smell loss ranging from total smell loss, known as
anosmia
, to three levels of partial smell loss, known as
hyposmia
. Similar tests were performed with the four known classes of tastes: salty, sweet, sour, and bitter, to classify taste loss ranging from total loss, known as
aguesia
, to three levels of partial taste loss, known as
hypoguesia
. In addition, some patients experience a distortion of their sense of taste and smell, known as
dysguesia
and
dysosmia
, respectively, in which smells and tastes that might be pleasing to the typical person may become very unpleasant.
This classification scheme became very useful as Dr. Henkin sought to better understand the causes of smell and taste loss and treat patients with these symptoms. The most common reasons people lose these senses include (a) inflammation of the nasal passageways known as
allergic rhinitis
or (b) following a viral infection or (c)
traumatic brain injury
. Over the course of the Clinics history, Dr. Henkin has observed that taste and smell loss are usually brought on by a response to one of these causes but persist long after the cause itself has disappeared. Given the apparent relationship of taste and smell loss to inflammation, Dr. Henkin hypothesized that each of these causes (allergic rhinitis, viral infection, or traumatic brain injury) interferes with the perception of smell by causing an imbalance between anti-inflammatory and pro-inflammatory factors called
cytokines
.
Testing The Hypothesis
To test his hypothesis, Dr. Henkin collected samples of patient blood, urine, saliva, and nasal mucus to test for a variety of biochemical compounds that might affect smell. Data collected from patients over the past forty years show a remarkably consistent pattern characterized by an imbalance in the secretion of cytokines involved in odor reception. Specifically, Dr. Henkin found higher levels of
anti-inflammatory cytokines
(called interleukin-1ra, interleukin-10) than
pro-inflammatory cytokines
(named interleukin-1α, interleukin-1β and tumor necrosis factor ) in patients with smell loss. These findings support Dr. Henkins hypothesis. Indeed, he has had success treating patients with a variety of therapies, all aimed at righting this imbalance and re-stimulating the growth of taste and odor receptors.
How We Smell
Lets see how we smell. Odors are received by smell receptors in the nose, located in the olfactory epithelium. These receptors normally grow, develop and die over a period of 1-30 days. They do not have blood vessels, but they are nourished by specialized proteins secreted into your snot or nasal mucus by serous glands in your nose.
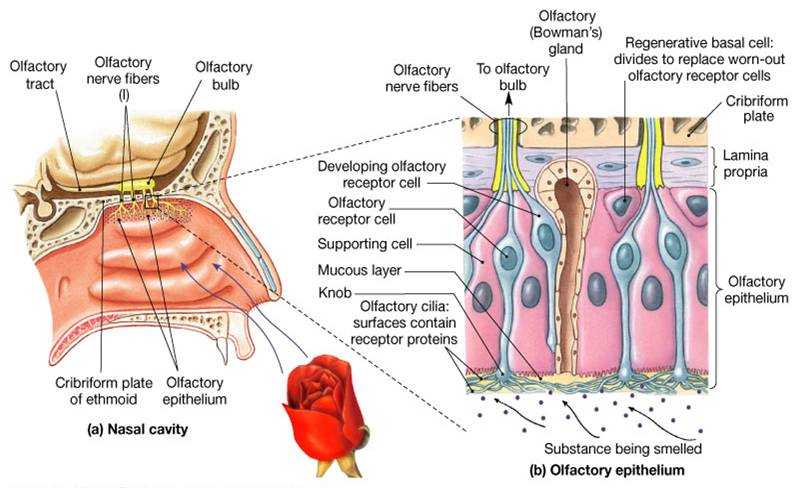
The Olfactory System.
When an illness or injury occurs causing loss of smell, the secretion of these nourishing proteins decreases and reduces the growth, development and function of these smell receptors in your nose. Dr. Henkin treats smell loss by restoring the balance of proteins and cytokines in nasal mucus. This often involves intranasal administration of drugs that will either inhibit or stimulate the factors that are out of balance. Restoring the balance of these chemicals corrects the receptor malfunction and the smell receptors begin to work again. As the smell receptors work, the ability to smell returns.
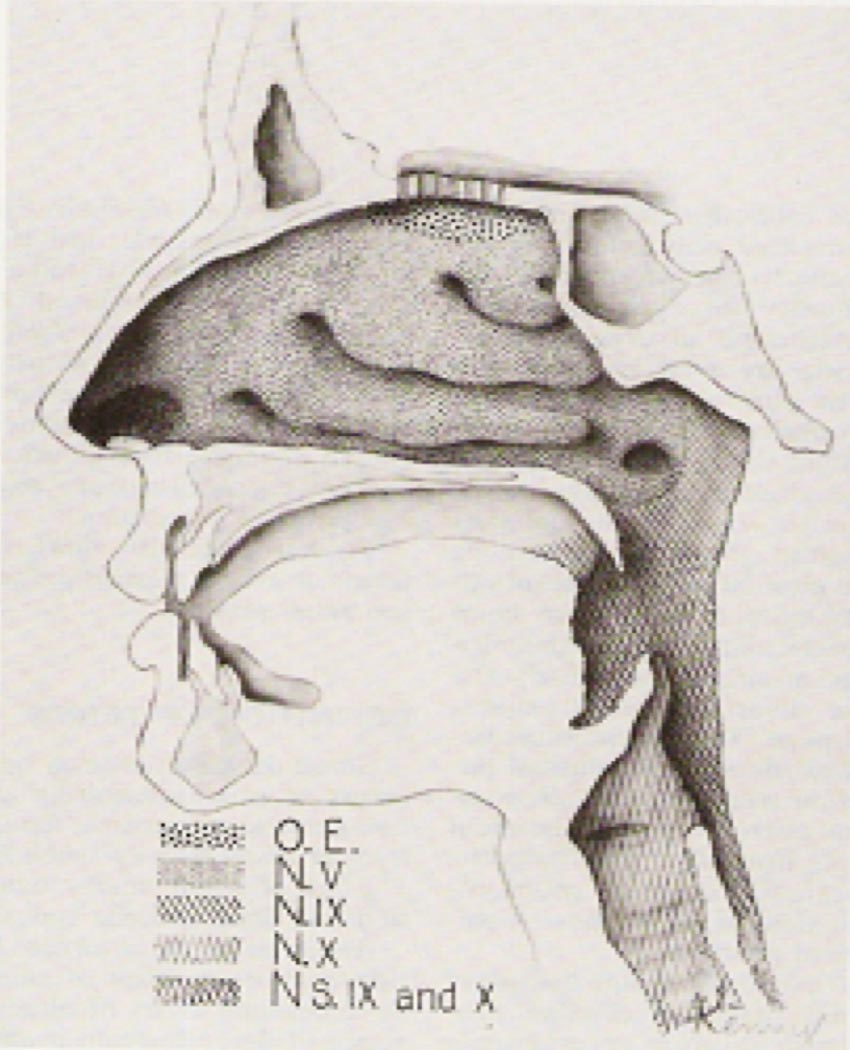
Gross Anatomy of Human Olfactory System
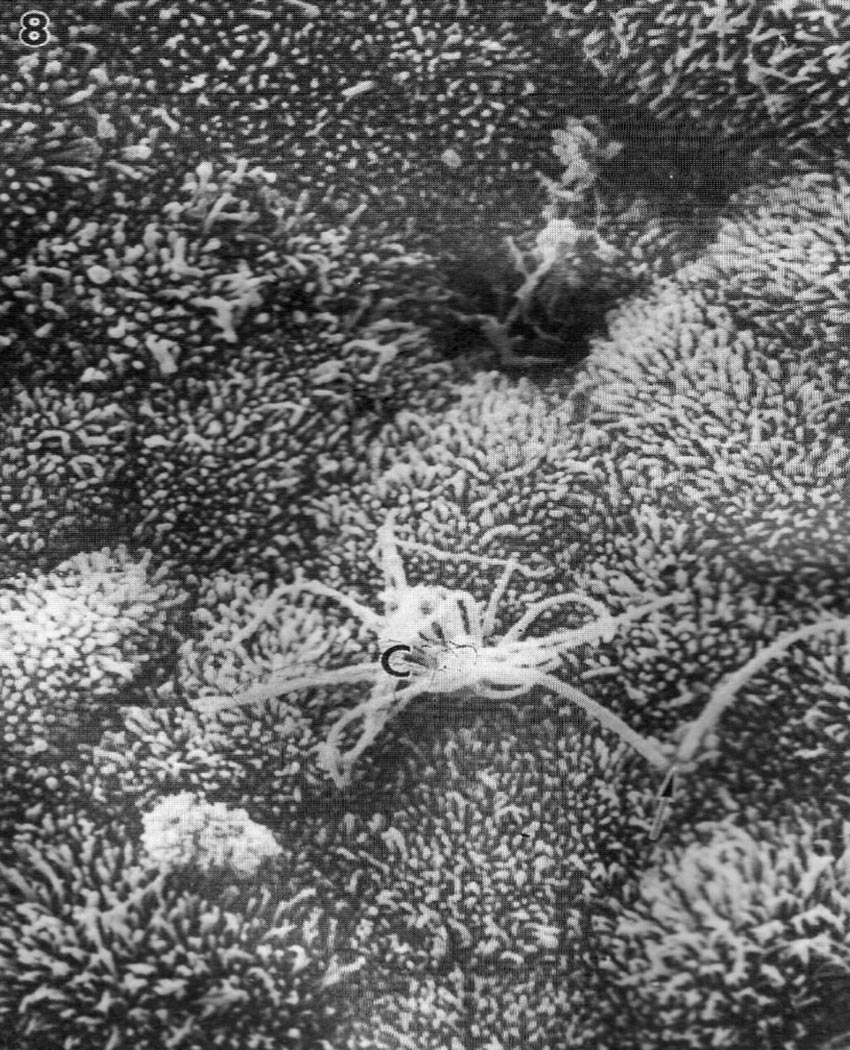
Scanning Electron Microscopy of Surface of Human Olfactory Epithelium
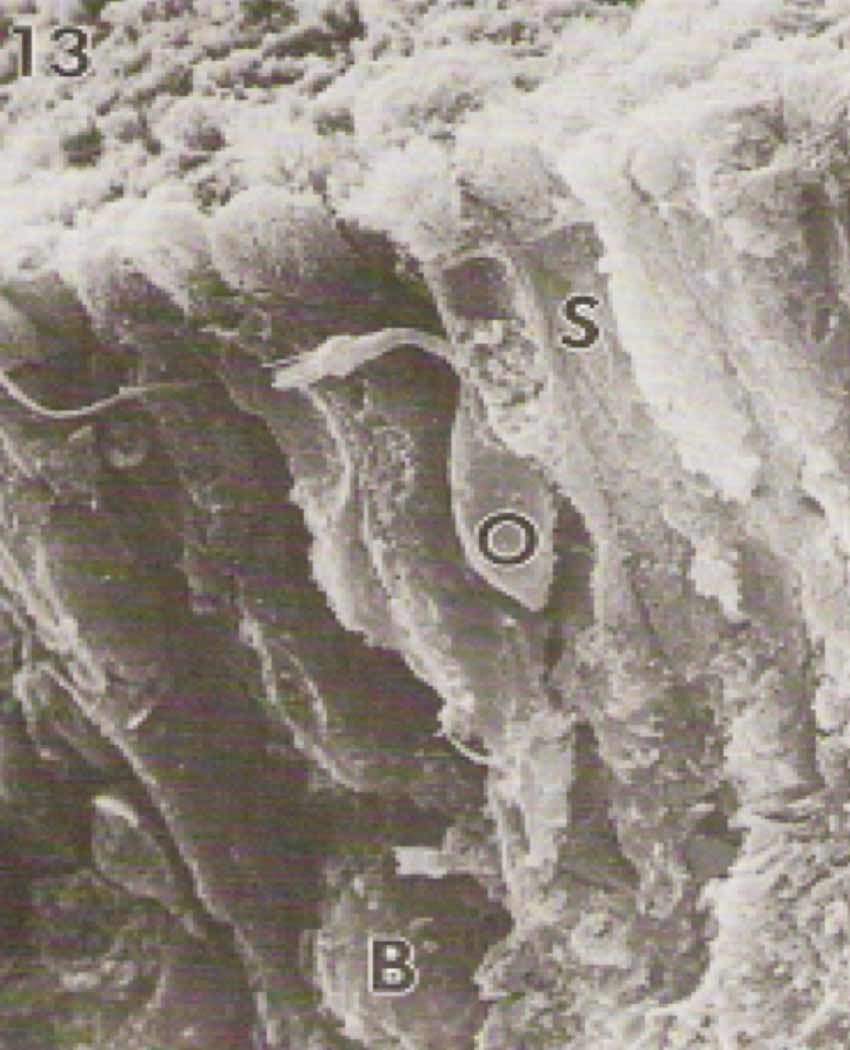
Scanning Electron Microscopy of Normal Human Olfactory Epithelium
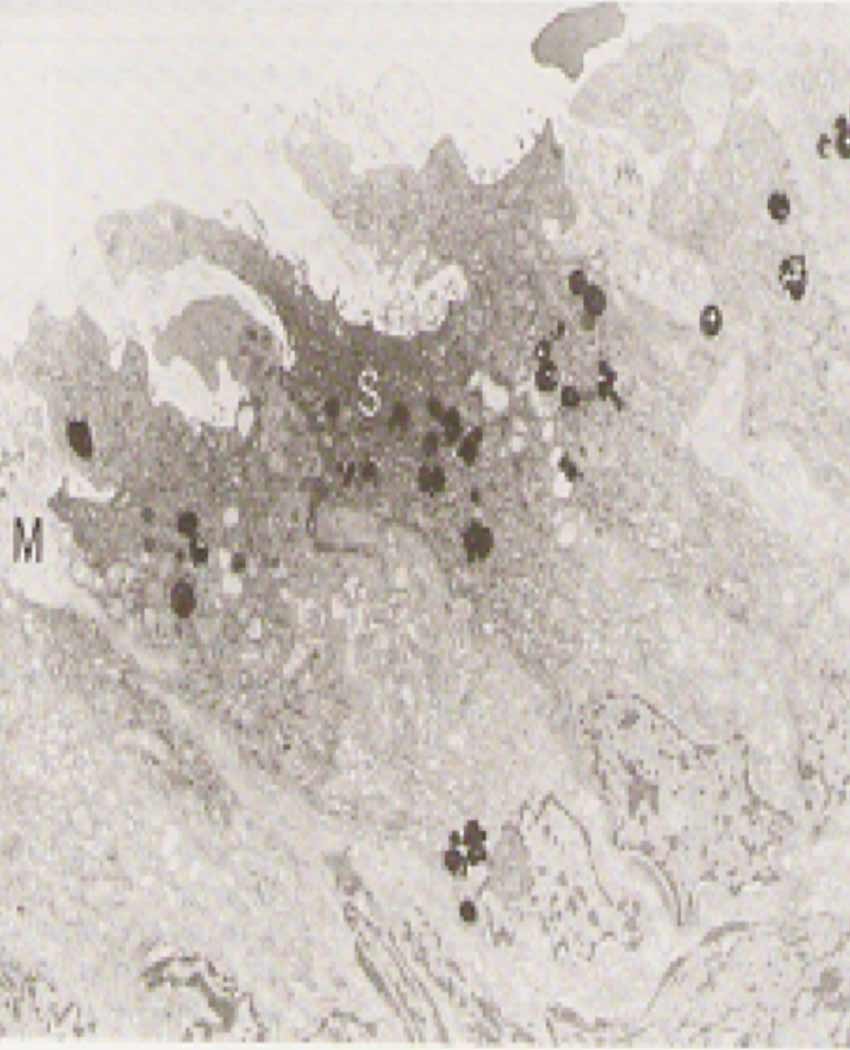
Electron Microscopy of Olfactory Epithelium of Patient With Hyposmia (Loss of Smell)
<Prev
Next>
Dr. Henkins accomplishments at the Taste and Smell Clinic have implications for a variety of disorders ranging from rheumatoid arthritis to neuropathy. Its all about the balance, explains Dr. Henkin. There are untold numbers of diseases caused by such an imbalance, and our ability to first recognize and then rectify these imbalances could improve the quality of life for millions of people.
Dr. Robert Henkin is the Director and Founder of the Taste and Smell Clinic located in Washington D.C. Over more than forty years at the Clinic, Dr. Henkin has helped thousands of patients regain their sense of smell and taste and become a pioneer in research on the topic. Prior to his transition to science and medicine, he was a musician who wrote music for Hollywood. He decided to pursue a second career in science because he was interested in how music affects our emotions. When not in the laboratory or seeing patients, he still writes and performs his music, although his influences and tastes have certainly changed over the years. He also enjoys farming.
To Learn More:
- Henkin, R. et al. 2013. Taste and smell function in chronic disease: A review of clinical and biohemial evaluations of taste and smell dysfunction in over 5000 patients at the Taste and Smell Clinic in Washington DC. American Journal of OtolaryngologyHead and Neck Medicine and Surgery.
- Henkin, R. et al. 2013. Cell signaling in smell loss (hyposmia). The FASEB Journal. 27:601.4.
- Henkin, R. 2013. Nasal mucus contains cAMP and cGMP which are critical factors in preservation of normal olfaction. The FASEB Journal. 27:1049.1.
For More Information:
- The Taste and Smell Clinic. http://www.tasteandsmell.com/clinical.htm
- Podcast: When the Sense of Smell Fails. http://lifelines.tv/when-the-sense-of-smell-fails
http://www.wvec.com/home/WVECnewsanchorseekstreatmenttoregainfullsenseofsmell-208293951.html
- Henkin RI, Levy L. 2013. Initiation of olfactory memory in patients after successful treatment of patients with congenital hyposmia the role of neuroplasticity. The FASEB Journal. 27:934.5.
- Henkin RI, Velicu I. 2012. Aetiological relationships of nasal mucosal cyclic nucleotides in patients with taste and smell dysfunction. Journal of Clinical Pathology . 65:447-451.
- Henkin RI, Velicu I. 2012. Etiological relationships of parotid saliva cyclic nucleotides in patients with taste and smell dysfunction.Archives of Oral Biology . 57:670-677.
Taste and Smell
- Senses and Perception. http://www.brainfacts.org/sensing-thinking-behaving/senses-and-perception/articles/2012/taste-and-smell/
- Taste and Smell. http://uconntasteandsmell.uchc.edu/facts/index.html
- The Surprising Impact of Taste and Smell. http://www.livescience.com/2737-surprising-impact-taste-smell.html
Anosmia and Aguesia
- Anosmia Foundation. http://www.anosmiafoundation.com/intro.shtml
- Taste disorders. http://www.nidcd.nih.gov/health/smelltaste/pages/taste.aspx
Hyposmia and Hypoguesia
- Smell disorders. http://www.nidcd.nih.gov/health/smelltaste/pages/smell.aspx
- Hyposmia. http://www.sensorysociety.org/ssp/wiki/Hyposmia/
Written by Rebecca Kranz with Andrea Gwosdow, PhD at www.gwosdow.com
HOME | ABOUT | ARCHIVES | TEACHERS | LINKS | CONTACT
All content on this site is © Massachusetts
Society for Medical Research or others. Please read our copyright
statement — it is important. |
|
|
Dr Henkin

What would it be like to live without being able to detect any odors? For one
thing, Thanksgiving would be much less enjoyable, perhaps disturbingly so
In this episode, we talk to Robert I. Henkin of the Taste
and Smell Clinic in Washington, D.C., who will tell us why people lose their
sense of smell and how his research can help some people restore it. (Begins
at: 02:03)
The Buzz in Physiology features studies on a
simple
test
that may determine arterial stiffness in adults older than 40, and a look
at a 1950s program that tested the
fitness
of women to become astronauts.
(Begins at: 00:43)

"Demystifying Medicine - Taste: good and bad"
Dr. Henkin's presentation at the National Institutes of Health.
Great Science Sites
NIH | High School
NIH | Middle School
ACS | Science for Kids
SciAm | Blog
Sign Up for our Monthly Announcement!
...or  subscribe to all of our stories! subscribe to all of our stories!

What A Year! is a project of the Massachusetts
Society for Medical Research.
|
|